

This is a fast forward through the slide set of a workshop on demand and capacity in healthcare. The story takes participants through some thinking tools for what demand and capacity actually mean in the real world and building a model that can be interpreted at any scale from an individual patient, to a single pathway, a service, or an entire population. The result is a sensemaking method of understanding how any particular type of work, works at a system level. The real trick is that the model is based on some sound systems science and recognises the tension between system constraints (structure of capacity) and dispositions (predictability of demand). Through this lens it becomes clear that nothing scales, you have to work at the right scale.
The model originated in 2004 within the development of a Paediatric demand and capacity tool called STEAM. This was further developed through national work on Care Planning in 2008, called Passing the Baton, together with the work of several practitioner led Communities of Practice. In 2010 the multi-agency Complex Care Forum was established to share research and practice in Multidisciplinary Working and further developed the model, creating a number of policies and practical examples of how to work in the complex space. This culminated in the development of the measurement device nicknamed ANGEL, deployed in several organisations.
The following is an extract from a discussion document that considers alternative methods of managing Flow in complex organisations, first published as ‘To Flow or Not to Flow’ Wyatt & Griffith (2012). It highlights some of the key concepts in making sense of the system and the development of methods and tools to put the ideas into practice. Since then, the model has been used to inform numerous small improvement projects, all the way up to the design of large scale Collaborative Commissioning Frameworks. The conceptual framework also informed the development of methods and tools that underpin the production and implementation of the Nurse Staffing Levels (Wales) Act 2016.
“… characterised as Flow”
There is a big problem in healthcare, although in the current climate, it may not be the one you’re thinking of. Across government departments, organisational boards, divisions, directorates, teams and individual practitioners, one particular problem seems to be keeping people busy above all others. It’s got many names, but is essentially all about how people access, move around and exit the service. The most common term for this problem is, “Flow”.
But Flow, isn’t actually the problem, or even really, a problem! The problem is in fact that few of the people who design services, have ever spent time to study the concept of Flow! Worse than that there are a few car factory fetishist arseholes, who think Flow is less important than than throughput, as if people are widgets. Throughput is another car factory nomenclature for describing the volume of profiteering shitbiscuits that splurges out of a thing, that doesn’t care. We are better than that.
As a result Flow is a word often mistakenly used in operational management to describe how one thing moves more quickly through other things around it, like the pace of water in a river. After all, water or any liquid for that matter is the substance most synonymous with the idea of Flow. However, Flow is not defined by the relative speed of the moving part, the water in the river or in healthcare, how quickly the patient moves around the hospital – their length of stay.
In the case of the river, the cause of the Flow is gravity, pulling constantly down on the body of water. The effect is the innate ability of water to effortlessly spread out and slide down the floor, following the path of least resistance. So, the water on its own will not just Flow. Gravity on its own does not Flow. The Flow is actually an observable product of both interacting.
Flow is a phenomenon that occurs when the causes and the effects of the movement, are in a particular type of relationship. The first thing to note is that a variety of parts that are connected in a moving relationship is scientifically known, as a system.
Within a system, and when particular conditions are right, you will observe a type of activity characterised as Flow.
@complexwales
“…balance of demand and capacity”
Depending on the thing that is causing the Flow and the environment it is flowing in, what the Flow consists of and how it behaves can be different. If the ground is level the river will meander and if the ground is steep the river cascades. In systems that contain people for example, Flow is not only a physical state like the river, but also a psychological state.

This dual nature is probably most widely observed in the field of professional sport. An elite athlete has a variety of abilities such as physical dexterity, muscular stamina, game awareness and a competitive temperament. But despite these inherent qualities, elite athletes do not spend much of their lives using these capacities to their fullest extent. That is, without the additional component of a competition or challenger. Occasionally in competition, athletes have a great day. Everything seems to come together and success appears to be effortless. When drawing upon all their talent in the right place at the right time, it all works. Within sport this is known as ‘being in the zone’, or ‘in full Flow’.
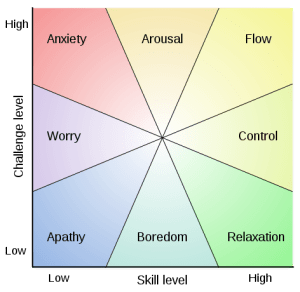
The phenomenon of achieving Flow to sustain relatively high levels of performance has been described by a number of experts. Most notably the adjacent diagram comes from ‘Flow: The Psychology of Optimal Experience’ (1990) by Professor Mihaly Csikszentmihalyi – pronounced check-sent-mar-HIGH-ay.
In an interview, Mihaly described Flow as “being completely involved in an activity for its own sake. The ego falls away. Time flies. Every action, movement, and thought follows inevitably from the previous one, like playing jazz. Your whole being is involved, and you’re using your skills to the utmost.”
To achieve a Flow state, a balance must be struck between the challenge of the task and the skill of the performer. If the task is too easy or too difficult, Flow cannot occur. Both skill level and challenge level must be matched and high; if skill and challenge are low and matched, then apathy results. Although principally a Psychologist, Mihaly’s model of challenge versus skill, is completely transferrable from mental to physical and from individual to systemic concepts of Flow.
In summary, Flow is the phenomena observed when there is a balance between the cause (challenge) and the effect (skill). The nature of the Flow will change along with the intensity of these two fundamental forces. In the case of healthcare, it is more common to call challenge, the demand placed on the system and skill, the capacity of that system to respond.
For Flow to exist there must be a mutual and continuous balance of demand and capacity.
@complexwales
“… looking back, it’s obvious”
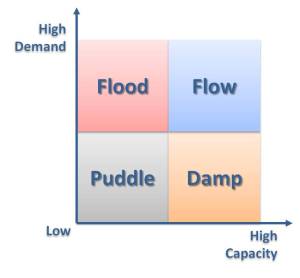
So for Flow to exist the demands and the capacity of the system (to deal with those demands) must be in a dynamic relationship. Taking the water metaphor a little deeper, the adjacent diagram displays this in a simplified relationship:
- Too low and the system is stagnant
- Too easy and the system is inefficient
- Too difficult and the
system is broken - In an active balance, there is Flow
Within healthcare it follows that demand represents the needs of the patient; and capacity, the ability of the organisation to adequately respond to that need. So what are the needs that the health service must be able to respond to?
This question is a wicked one. Historically it has been answered by focussing on the ‘patient’s problem’; their diagnosis or even the prescribed treatment, as a description of the demand. However over the past couple of decades the demands placed on healthcare have changed. Not just in volume, more of one to less of another, but in the nature of the need itself.

This change has been recognised, researched and described by many commentators, including Dr Trisha Greenhalgh et al in a series of articles in the British Medical Journal in 2001. Commencing with “the challenge of complexity in healthcare”, Volume 323 15/09/2001, this and three succeeding articles each week, challenged the validity of problem oriented ideas, structures and practices.
In essence the argument suggests that medical education, clinical professions and healthcare in general, have sought to improve and develop services on a speciality based model. Thus from early in a clinician’s career a choice is required, as to which aspect of care they wish to focus on. These aspects are typically categorised into technical fields or Colleges working on discrete functions, parts of the body, on specific diseases or even in specific delivery models (Day Theatre, Primary Care). Practitioners are taught, employed and developed to become increasingly technically sophisticated in their field.
Meanwhile, the needs of the population have changed along with their expectations of service purpose and quality. Fewer and fewer people now access healthcare with a single problem, requiring a single treatment, in a discrete episode of care. Increasing numbers of people now have multifactorial problems. More than one long term condition, social, psychological and environmental factors all combine to challenge the effectiveness of those historically discrete treatments. In other words, the caseload has become complex.
As a result defining demand simply by one problem or one perspective on a person’s situation, becomes at best incomplete and at worst, a dangerous oversimplification. Recognising a single discrete problem, making an accurate diagnosis and responding with a definitive treatment, is correct and effective, when there is only one or maybe two issues to consider. Often there is a comprehensive and reliable evidence base for such activity.
However, when a person presents with a number of related factors that affect their typical life, then those factors and the relationship between them, will be sensitive to change over time. How addressing one factor may affect the other factors, is often difficult if not impossible to predict. Although it may still be necessary to undertake a defined treatment, in addition, the practitioner must now consider the person holistically and continually.
The most significant benefit of considering Flow as a system is that of scalability. In viewing relationships of demand and capacity as a system, it is possible to use exactly the same model to consider systems at very different scales, from the smallest individual action to the largest societal impact.
Mihaly’s original concept of demand versus capacity identified Flow for an individual, corresponding to that person’s own individual goals, drive, or preferences. Therefore, the sections of the diagram were annotated or worded from the perspective of an individual performer and unchallenging situations were given negative connotations. However, what doesn’t challenge one person, and therefore appears boring, may be perfectly aligned to another person’s interests and talent. Clearly at a system level considering Flow on a single two dimensional chart requires interpretation and contextualisation, on the wider scale.
For example, a nurse on a ward would be quite comfortable surrounded by six different professions, working on an unconscious man with a heart condition, who is sedated and attached to several machines, bleeping and displaying a variety of numbers and charts. A few months later, a different but equally skilled nurse in a residential home is helping the same man – who just happens to have a learning disability – to recognise his feelings of anger and anxiety and choose not to punch a housemate in the face for using his Marmite.

In all seriousness, these two situations represent two different types of service, each with its own demands and capacities. Swap these two nurses and what was fun for one, is boring for the other and conversely what is routine for one, could be an anxious mess for the other.
Mirroring the nursing analogy above, each of the four corners are systems in their own right. The ward nurse may be considered working in a ‘Low x High’ system: dealing with a common situation using standard technical interventions. The LD nurse would represent a ‘High x Low’ system: dealing with a uncommon situation with a personalised albeit equally skilled intervention. Similarly, each of the four types can be considered perfectly designed, to deal with those specific different types of challenge versus skill and containing their own relative Flows.

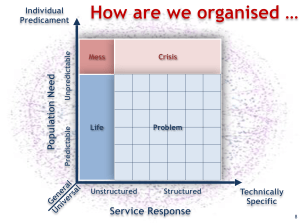
From the original model, the negative connotations of low levels of challenge and skill are reinterpreted systemically using the same axis as before, the diagram has challenge on the vertical axis, entitled “increasingly unpredictable life” and skill on the horizontal axis entitled “increasingly structured intervention”.
Subsequently, in modelling of Flow as demand versus capacity, the chart is first reduced to its most basic constituent relationships: that is, high and low specificity of each axis compared to that of the other, in a classic quadrant plot. Note that in this sense demand and capacity are not simply a measure of size or volume.
This quadrant model is a horrible oversimplification, but one that can be used to consider the structure of the whole health system. For the purposes of a very simple thought experiment, the main overarching service types within the existing system can therefore be identified and grouped into the four principal categories of Flow:
| Collective Support ________________ Predictable Unstructured (A life to get on with) | Collective Support is the kind of care that is often invisible in modern life, that is, until it’s suddenly not there. They are ordinary societal services that help us live our lives that are taken for granted, eg street lighting, road signs, public sanitation, environmental safety, access to food, information, leisure and shopping. The range extends from these invisible aids through to more traditionally recognised support in frontline health care and social services that mostly help disadvantaged people to fulfil the normal activities of daily living. |
| Pathway Services _______________ Predictable Structured (A problem for us to solve) | Pathway describes the traditional majority of health and social care services that we have come to rely upon. From adult social care, housing and variety of health services based around solving an identified problem, whether that’s reading and writing, a dentist, feeling unwell or even chronic disease. This is also how we have built and subdivided our large institutions such as hospitals, split into diagnostic or professional groupings. And for what it does, this is a good thing. Most of our progress over the last 100 years has come from this model of increasing specialisation (see Greenhalgh) |
| Urgent Care ________________ Unpredictable Structured (A crisis to overcome) | Urgent Care systems have built up from the pathway model but where an individual diagnosis doesn’t necessarily take precedent. The person’s life is unpredictable perhaps to the point of crisis, where the work focuses high levels of expertise and resource, to saving life or preserving long term wellbeing. At one end these services are the Emergencies and A&E where save life and do it quickly, are the norm. It also includes very special places such as emergency theatres and intensive care, where the initial injury is actually secondary to the goal of keeping you alive and safe. |
| Search & Rescue _______________ Unpredictable Unstructured (A mess to clean up) | This type of care is mostly seen in fields dealing with interagency health and wellbeing such as child protection, disabilities, mental health and other long term life-limiting problems that include homelessness, poverty and social isolation. The biggest problem to begin with, is that these people are lost to the system, we don’t know who or where they are. When found, the intervention is holistic case management, but initially the person’s typical life may remain prone to rapid and significant change. They don’t necessarily have a single technical problem to fix and are more likely to have many small, interrelated challenges that they live with and making them immediately vulnerable or at high risk of harm. Life threatening situations are never far away. This also includes more traditional severe harm for example, where someone has bounced off their motorbike and has yet to be found. |
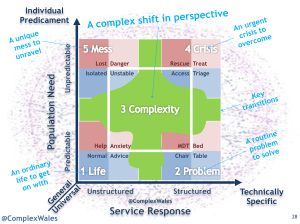
Clearly these four categories are a convenient approximation and some services may consider themselves to sit on the boundary between groups. It is immediately obvious therefore, that the boundaries are blurred rather than highly specified. However, in broad terms these are the four kinds of services that our traditional systems contain and the four broad categories of capacity with which we attempt to meet demand, evident in most organisational policies. From the resulting model, each one of these categories can similarly be mapped in terms of the range of demands placed upon them and their capacities to deal with those demands. But the really useful insight comes when these 4 service groups are placed together and considered as a single dynamic, whole system.
The model diagram has been resized to visualise the proportions of the system occupied by the 4 main types of service in resource terms. The Life is squashed into relatively generalised work albeit supporting people with increasingly unpredictable lives (15%). The majority of services are chopped up and structured into Problem units (60%), some special services rise out of that in Crisis (15%) and as we know around £1 in every £10 in healthcare is spent on finding and helping people in a Mess (10%). This is how the healthcare systems have been traditionally structured.

Meanwhile, practice develops and those procedures that used to be in theatre, are now used on the ward, those on the ward are in outpatients and work that used to be special is now on the High Street. Different types of crisis services have been set up to do more ordinary things; more Life-style services are commissioned to compensate for rationed access to Problem solving; and anybody who doesn’t fit, has to have a vastly over complicated unified assessment, a multiagency case conference and a highly specified care package commissioned through a European Tender, regulated by a new national unit. An exaggeration perhaps, but a valid description of a traditional and common structure, that is no longer fit for purpose.
The result is that services specify what they are for, to maintain control over demand. Rational criteria now determine what type of demand is permitted in and the capacity to deal with it is structured into tightly monitored separate pathways. When patients need a type of service they are referred, transferred and discharged to align with the structure and comply with the bureaucracy invented to manage the rationing across all those little boxes! The trouble is of course that the demand has become more complex. A person may need one type of service this week and a different one next week. The new transactional structures cannot respond quickly so; the Cardiology Ward is full of people who don’t need to be there, the A&E is swamped with people with simple Problems and the process for sorting out the Mess people end up in, has run out of money.

We are left with a cohort of patients in the middle with a range of needs that will shift over time, who therefore don’t fit anywhere in particular. They are effectively left in ‘nomansland’ despite actually being located in all four of the traditional services, possibly at the same time. This kind of shift in demand requires a complex adaptive route through the systems so that as needs change, demands are identified and services respond at the right time and in the right way. That’s called Adaptive Capacity.
When considering the clinical research identifying the emerging complexity of care and putting that in the context of a vast traditionally structured and fragmented Health and Social Care System; we have a gaping hole in the middle, full of people who no longer fit.
The structure of our system is not designed to deal with complex Flow and looking back, it’s obvious.
@complexwales
“… one unit of Capacity”
In considering the relationship of demand and capacity, in context of the environment or structure through which it Flows – our care system is clearly not just one type of system.
There is now an established global field in the scientific exploration and understanding of how systems work. Over the past 50 years in particular, this relatively new area of science has been validated with both academic research and successful organisational applications across many industries. Perhaps most significantly within these developments is recognition of the effect of layering: of systems within systems. Particularly within big institutions and large scale issues such as social policy, this concept of Nested Systems, is being recognised and becoming much better understood. There are various systemic frameworks within Complexity and Systems Science similar to Mihaly’s dynamic model, that attempt to explain the principle characteristics of different types of system and their inherent Flows. In short, the sustainable ones are based on networks not hierarchies.
Each model is derived for a different purpose, from the same General Systems Theory that describes a range or, continuum of system archetypes; from ordered and predictable at one end; through levels of abstraction; to unordered and unpredictable at the other. In the context of healthcare, at one end there are people with simple problems for which there are simple, predictable, evidence based solutions. At the other end there is a person whose life may be critically unpredictable and one that no single practitioner should attempt to deal with in isolation. Tools and techniques that are successful at one end of this continuum are not as effective at another. Therefore, the way we manage our health and care services must similarly reflect this range of demands, with a complementary range of capacities.
In considering Flow as a product of the system, it becomes clear that within any organisation the patterns of demand versus capacity will be different, depending on the situation. The system must therefore, encompass a similarly wide range of working methods and practices. This means that the characteristics of the environment, the nature of the external demands and the internal capacities, can vary sufficiently, to be able to distinguish and define a range of systemic Archetypes and corresponding Flows across each organisation. Go with it, we’re pushing the envelope on the Flow metaphor.
1. Life in the River.
System Type
Essential (Life)
This is the type of Flow that mostly goes
unnoticed, where
many ordinary
elements of work or life simply tick over, or do what they are
supposed to. Cause
and effects are
obvious, linear and
predictable and there
is no need to enforce
controls to achieve a natural Flow.
Working Principle
Common Practice
The type of demand is
easily recognisable
and readily
categorised. The
corresponding
capacity is perfectly
aligned to achieve the
same outcome reliably and consistently. Eg Record a standard
set of observations
Flow Metaphor
The River
It could be a stream or torrent and you may use the river for various purposes, take a dip, go fishing, wade across it, build a bridge over it or go around it, but
essentially there’s no
need to stop it
continuing on its
natural course.
Sustaining the natural
order of thing works
best.
2. Problem in the Dam.
System Type
Expert (Problem)
This type of Flow occurs when natural processes combine, or are deliberately lined up in a planned sequence. Cause and effect relationships remain linear, but now a number of factors have to be considered to make accurate predictions and plan accordingly.
Working Principle
Good Practice
Specific expertise is needed to accurately calculate the demand and navigate the pathway. Capacity is specified from a limited range of options and deployed within the pathway to achieve a short term goal. Eg Agree when to do which set of observations.
Flow Metaphor
The Dam
This is about people deliberately stopping the natural flow for a specific purpose. Constraints are calculated and mechanisms designed to temporarily control the Flow: pumps, waterwheels, pipes, canals and lock gates. Eventually the water still reaches the sea.
3. Shift in the Tide.
System Type
Complex (Shift)
This type of Flow occurs when some or all of the factors at play are changing in real time. Cause and effect relationships are indirect, not fully understood from the beginning and from small changes new patterns will emerge over time.
Working Principle
Emergent Practice
The demand is partially unknown and variable, like a prognosis, the capacity to respond must adapt quickly as greater understanding is built through continuous feedback. Eg Recognising and dealing with the changes in observations.
Flow Metaphor
The Tide
It is impossible to control the Flow, but you can choose to work with it. There are recognisable patterns and so successfully navigating the tide requires skill and judgement in real time, on the boat so to speak, from an experienced pilot, not just a chart.
4. Crisis in the Weather.
System Type
Tactical (Crisis)
This type of Flow occurs where the relationship of cause and effect is ambiguous and contingencies must be identified in advance of need. Although you can imagine what patterns of cause and effects will materialise, you don’t know exactly when or where those situations will arise.
Working Principle
Novel Practice
This is preparation for demands that are unpredictable but foreseeable. You can anticipate problems, and identify scenarios for which the right response or capacity is prepared, but deployed only when circumstances dictate. Eg Predicting what the change in observations may lead to.
Flow Metaphor
The Weather
You know that it’s warmer in the summer, it is going to rain, water levels could rise or fall and you cannot control it all, so you prepare. Buy wellingtons, don’t build on flood-planes, do build lighthouses on foggy rocks and set up rescue services for when it inevitably all goes wrong.
5. Mess in the Ocean.
System Type
Chaotic (Mess)
This final type of Flow occurs, when several patterns conflate in unpredictable ways. Causes and effects, demands and capacities, become entangled in such a way that it is impossible to reverse or disentangle the components. Small differences in initial conditions create very different final outcomes.
Working Principle
Bespoke Practice
Try and deal with demand in the same way twice and you get two completely different results. Normal rules of work are usually ineffective or mostly ignored in favour of a small number of core principles such as “protect the vulnerable”. Eg Intervening successfully in the absence of prior observations.
Flow Metaphor
The Ocean
Despite all the knowledge and experience available, sometimes there are extraordinary events. A river floods, the lock gates break and your boat is pushed into the seasonal tides, towards a weather front driving deep ocean currents that carry you out to sea. In the middle of the Ocean, there’s no choice but to go with what you got.
This table is not intended to define every conceivable pattern or describe a single theory of Flow. It is however a distillation of the range of scientific system archetypes. From essential ordered to chaotic unordered, the systems are organised into five broadly recognisable and distinct groups that is mirrored in the previous analysis of organisational structure. It is a tool with which to recognise which type of system you’re in, understand the characteristics of Flow and subsequently know which type of work, works.

A longstanding organisational axiom is that the only alternative to top down control and the imposition of order (a Pathway) is, the inevitable fall into chaos and anarchy (a Mess). Ironically, treating one as if it were the other causes most of the problems. The systems approach, challenges this convention with a continuum of scalable complex and adaptable methods of working in between: the diagonal from bottom left (Life) through the middle (Shift) to top right (Crisis). These nested systems have proven to be a much more common and accurate description of typical life and work, than merely the two competing extremes.
On this note, the most important point to remember is that none of these characterised systems are in any way better or worse than any other. Neither are they somehow ranked in a hierarchy of increasingly better types of system or methods of creating Flow. Working successfully in each type of system, with each type of Flow, is equally challenging for different reasons and each method of working has a different range of tools, techniques, skills and knowledge that are effective in context.
In considering one extreme as an example, it is common for chaos to be synonymous with a harmful crisis or a terrible event. However, the basic nature of a chaotic system is not bad, it is just uniquely unpredictable. Good and bad events and outcomes may exist side by side and repeating the same actions, may lead to completely different outcomes the next time:
“A minor solar flare happens to hit the earth just as the North Atlantic jet stream comes into view of the sun. The jet stream turns slightly further south and the UK gets hit by a period of winter snow from the east. The European weather system is nudged southwards and cold air is pushed over Spain, getting all mixed up with the humid hot air. A thunderstorm erupts and tips a month’s rain in under an hour onto a dry mountain. Further down the valley, lightning ignites a wildfire which the storm blows eastward, towards a small town on the banks of a river. The wild fire is trapped by the swollen river and burns itself out, to be finally doused using pumps and tractors from a nearby vineyard. A year later the Rioja from that little town has a fabulous smoky undertone.”
This may seem a strange little story at first, but it is meant to illustrate the unpredictability of some types of Flow. Many similar analogies exist, loosely describing a phenomenon popularly called the ‘butterfly effect’. From the beginning, the outcome could not have been predicted however, with hindsight, the sequence of events appears coherent and rational.
What this means is, as the system becomes less predictable and structured, what has happened before, becomes a less and less successful predictor of what may happen next. In chaotic flows, hindsight does not lead to foresight. The nature of demand and the range of capacity required to deal with it, is also different from situations that predictably repeat with high reliability. Subsequently, the relationship of demand and capacity cannot be defined as simply a measure of size, speed or volume, the number of referrals or worse the number of bits of equipment available.
The fundamental systemic issue is that there is more than one type of flow and as a result, one person does not equal one unit of demand and one appointment, does not equal one unit of capacity.
@complexwales
“… this kind of demand?”
Across health and social care organisations, most services have traditionally captured vast quantities of categorised data about every individual bit of a person that can go wrong. More recently, computerised information systems have expanded beyond this diagnostic model to aggregate clinical and logistical activity in an increasingly comprehensive and granular dataset.
Concurrently, individual practitioners in a wide range of services have been slowly moving away from a purely problem based structure, to a more holistic bio-psycho-social model, as identified in a considerably growing source of research and practice literature. Information systems, for the most part, have not kept pace with this move toward integrated practice and as a result, most modern healthcare organisations have to some extent, become data rich and knowledge poor. The management and clinical practices appear to have diverged.
Recognising the new complex demands and the divergence from traditional organisational models; it is a reasonable conclusion that new or different tools and techniques are required to design, nurture and deploy the necessary capacity, to recognise and respond effectively, to the changing demands. As such, new methods and tools for modelling demand and capacity are required, but before we can get anywhere near a coherent approach for this shifting environment, we need to revolutionise the way that we monitor and measure complex living systems like healthcare.
From small individual projects, to national collaborative commissioning frameworks, the same question is being asked; how to do I create the right kind of adaptive capacity to deal with this kind of shifting demand?
@complexwales
An invitation…
The further development work highlighted in the introduction, has sought to create meaningful ways to engage with front line staff and design and apply new systems of working based on the complexity paradigm. This work is centred around really understanding demand and capacity and includes research and development using ANGEL, coproduction of the Collaborative Commissioning Frameworks and widespread workforce engagement for example, in embedding nurse staffing legislation into everyday practice.
If you’d like to see the workshop from the video in action, or run one for your team, simply get in touch. If you are interested in any of the concepts, methods and tools, or want to get a feel for how they’ve been developed and applied, ping us on Twitter. Always open for a coffee and a natter, but boy, can we natter.
| Matt Wyatt Advisor @ComplexWales | Susan Griffith Physiotherapist @SusanGriffith |
©Copyright 2012
