
I’ve spent most of my career in an around clinical decision making and the management of the knowledge, constantly orbiting around those often innocuous and sometimes critical, moments of decision. As a ‘non-clinician’ I’ve naturally got a certain objectivity to both the process and the content as critical bits of information are collated, dis-aggregated, critiqued, recombined and deployed to justify, the next best step. Although we keep an eye on a longer term goal, this is the timescale of most clinical practice, taking each step as it comes, in a form of successive limited comparison.
I’m deliberately saying information not data, in an allusion to some sort of precontemplative aggregation of the fundamental units of transmission. Saying that, empiricism is easy to practice but hard to articulate and as a result, I’ve constantly smashed my own forehead against the world of Information Communication Management and Technology (let’s call it IT).
Playing the part of operational translator, I’ve worked with and headbutted up against some brilliant IT people. Respect where respect is due; in most institutions they are brain-cuffed by various vacuous committees that seem more concerned with feeding the corporate beast than augmenting the actual work.
There are some glorious exceptions, but most of IT, is operationally curtailed by Leaderists whose thinking was carved onto stone, a long time before personal computers were invented, let alone ubiquitous and in the palm of your hand. That’s a blog for another day, but in short, our information structures are as fragmented, as our hierarchical ones.
I bear the scars on my forehead to prove it, as my management practice and research over the past 25 years, has felt as though it spanned the entirety of human evolution, when it comes to clinical information. I’ve joined deep dives into everything from health literacy, through prevention, onto routine primary, community, acute and intensive care, all the way to supra-regional emergency response.
Most of which, has stayed firmly on the left hand side of that picture. Everyone describes their information needs in different ways; have inherited a lexicon that’s etymologically lost in the midst of time; often mix common and technical usages; and offer little recognition or even respect for, the way others say things. It’s a touchy subject, mostly because of how hard you have to work and how long it takes, to change the simplest things. Because of this difficulty, people have become very temperamental about their own patch and quite rightly.
Well at least it’s difficult, when there’s not a pandemic to deal with. It’s been absolutely fascinating to watch the various physical and technological developments that have been ‘in committee’ for years, suddenly being made available to staff and the public, within a few days.
There’s never a better time to fix something, than when, it’s properly broken.
In a crisis the usual rules are null and void and you can do some of your best and worst work, all at the same time. But as a crisis begins to unfold there are discernible patterns and a sweet spot, where you can act Tactically to achieve considerable gains, with very little effort.
My friend @whatsthepont has blogged about this and a few of us like-minded souls are already working on capturing these opportunities, before they disappear into the foggy despair of a retrospective review. So, in a crisis, the real trick is to make sure that you choose to do the right thing, at the right time and record it, as you go along.
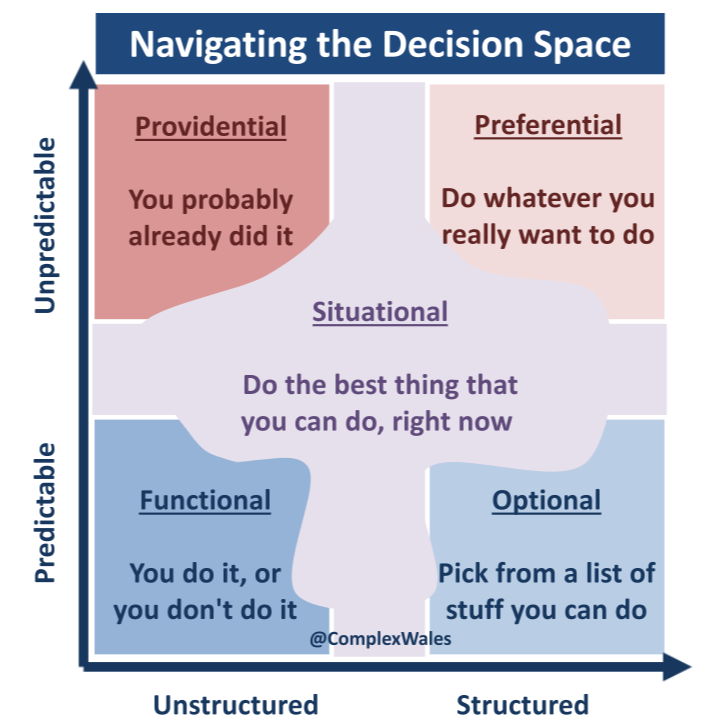
Contrary to the popular axiom, expertise does not enable you to ask a better question; it simply articulates, an annoyingly more specific one (bottom right). But there is a clear and present danger for people who do ask good questions, in flying off with the first answer that comes back (top left). No doubt amidst the chaos that’s reasonable, as you will be relying to some degree, on luck. But Tactics (top right) are all about experience, not expertise and making informed albeit reasonable choices in the face of uncertainty: what is it that given the opportunity, you would prefer to do?
In this liminal space (as Dave Snowden refers to it) where you’re not completely in chaos, but yet to establish entirely what’s going on, there’s a fine line. Can you take an informed preference and potentially innovate, or are you about to throw the baby out with bath water, only to try and relearn everything again, from scratch, in a hurry (bottom left)?
The Handover…
Before we start, I’ve been in this territory for a long time: from investigating critical incidents last century; to inventing this; then producing that; and so much more in the many years since that has made the title imagery to this blog as symbolic now, as it was then. So pay attention!
One thing I have learned over and over again, is that in reality clinical decision making follows pretty much the same structure, everywhere. Depending on the context, the decisions are framed in different ways, with differing depths of detail and with differing intentions, but the pattern, at least in terms of the information requirement, is the same. Sadly, you would not believe how many different places hold information independently from everyone else, all in slightly different shapes and sizes.
I once did a forensic audit of Child Health Information in a single community, and found 42 separate places holding unilateral data on the same child. Crazy and as a result very similar documentation and information gathering activities were being started from scratch over and over and over again, for no reason, and most importantly in the absence of, any single version of the truth.
I’ve lost count of the workshops I’ve been asked to run in various departments, where we’ve interrogated logic tables, printed off screen shots, taken apart policies and procedures and physically cut up standard documentation to make sense of the information requirement. After spreading everything out, what happens next has become boring. Bit by bit everything gets shuffled into a couple of piles of stuff recording the same thing. It’s literally exactly the same 5 dimensions, every time, even when during the process, I say nothing at all:
- Information about the Person: 10%
- Who are they, where do they hang out and what are their typical activities of daily life: their history, routines and the background that got them there.
- Information about Problems: 50%
- What’s the patient’s clinical disposition, how are they now and have they hit any diagnostic triggers for assessment: what’s wrong, to what degree and with what effect.
- Information about Direction: 5%
- Why are we doing what, who’s shared in which decisions and what’s the prognosis: what’s the goal, for which problem and to what level of achievement.
- Information about Work: 30%
- Where are we now, who’s in charge of the next step and what’s the expected escalation of Care: the plan, critical factors to watch out for and the process for review.
- Information about Continuity: 5%
- When do things need to get done, for the next handover or transfer of care and what’s the latest answer to the big question: from where, to where, by when?
Whether it’s on the phone in a first contact centre, with a telephonist with minimal clinical skills following a computer algorithm, or in a formal multidisciplinary meeting with a dozen professions debating the most complex and rare case – or anything in between for that matter – they are all typically attempting to agree upon, the next best step. This is not to belittle the fabulous MDT, or mount inordinate pressure on the telephonist, but to explain a commonality in their practice: that in the end, the people at the centre of those decisions, have a great deal in common and all want to know: from where to where, by when?
Each decision point attempts to create a picture of the patient to validate the answer to that question. To begin with, it’s the person themselves (as they are becoming a patient) who holds all the cards as they have most of the information necessary to make a decision.

So the picture of the patient, that the telephonist creates in a brief conversation with the person or their family, can be little more than a pencil sketch. Accurate enough in all five dimensions, to determine the next best step, but not containing any detail in terms of colour and texture.
This first form of Handover between a patient themselves and a professional, is mostly referred to as Triage and typically undertaken by people like GPs, Paramedics and Nurses in an ED (usually working from a broom cupboard, under the stairs, in the hall, by the front door).
The MDT also does Triage, but should begin their conversation with a detailed and colourful, albeit incomplete, rich picture of the patient. The information held by the patient, in terms of their wants, needs and aspirations, is still at the heart of the picture (it’s layout), but now there’s a flourish of additional experiential and technical detail: both in terms of the creation of the picture so far; but also the concepts, methods and tools best placed to enhance the picture further.
One of the best MDTs I’ve helped, used a little numerical code at the start when discussing a patient. I heard one patient denoted as “12” and then another patient got “46”. I asked at the end what the little numerical code meant and Prof chuckled before saying, “it’s the height of the patient’s notes in inches… the size gives everyone a shared sense of the history”. Abstract but meaningful, it was a form of painting by numbers that opened up a whole world of research for me that resulted in ANGEL.
Obviously, Handovers don’t just happen between departments. Anything up to four times a day, the staff in any single department change shift and Hand-Over an update on the current caseload to one and other. I’ve seen some pretty dire attempts at Handover that amount to little more than moaning from rushed scribbles, on sticky notes. Fortunately that’s very rare.
The best Handovers are succinct, sincere and specific and most importantly are a dialogue not a monologue. For a few moments the staff involved, paint the picture together. Noting the recent changes, the next part of the picture to work on and for a few moments painting together to add a few more lines and strokes to the picture: those chosen with care, to enable the next shift to continue to paint. I hope this ‘painting a picture’ analogy is working!
BUT and that’s a big but, most of that marvellous exchange simply evaporates into the ether and is rarely recorded anywhere, let alone digitally. But perhaps more infuriatingly, there is no reason that a Handover between departments should be any less proficient than the best between shifts, in ensuring there is complete continuity of care:
SUCCINCT: Clinical staff seem to abhor a space on a piece of paper, they are driven to fill every box, mostly out of fear that their organisation will blame them for some minor discrepancy, should anything untoward happen. Decision making is not like documentation, you need just enough information to evidence the decision. This is called the Rule of Sufficiency.
SINCERE: Those conducting handover, must really know their patients, not just possess data. In doing so, they can independently form their own honest opinion, prior to sharing it openly. Say what you truly believe, not just what you think you’re supposed to say. This enables people to spot misconceptions and critically assimilate information as it’s transmitted. Empirically, the best test for an honest decision is to go nose to nose with another person, with a second opinion. If two people independently come to the same conclusion, you’ve just halved the risk. This is called the Rule of Authenticity.
SPECIFIC: Get the first two right and this one is a piece of cake. And by the way, cake always makes for a better handover; it’s an emotional business. Don’t waffle or be vague, say the right things in the simplest of terms, that have been done and that need to be done. This can include very technical information and detail as required, but be precise as this is essentially the next best step that should carry you through to the next best decision. This is called the Rule of Validity.
Those rules are written about in both education and law, as the way to evaluate the quality of evidence. There is also a Rule of Currency, whereby evidence is time sensitive and at the moment of decision, had not been superseded. That is essentially the purpose of a Handover, to make sure everyone who needs to be, is up to date.
The Headache…
On every step of a patient’s experience through care, each person they meet at each place they occupy, attempt to paint that same picture. Everyone does their own form of Triage. The sad truth of it, unfortunately, is it’s not uncommon, for every place to start again, with their own pencil. That’s not too bad, you may think, as each place and practitioner gets to learn all about the patient from scratch and that’s got to help to develop the necessary therapeutic relationship: to really understand the patient and their wants, needs and aspirations. Yes, well all very nice but, in all living systems, context is everything.
In some parts of our business, the patients really don’t give a shit about getting to know us, you can stick your shared decision making where the sun don’t shine and they really really couldn’t care whether you smile and tell them your name… “just stitch the bloody leg back on”.
@complexwales
Ok, so I’m poking fun at the process a little, but every step of that story has different people, different paperwork and different computers that each stop at their own door. I’ve done plenty of patient follows in unscheduled care and it’s pretty common for one patient to receive care from 100+ people and 20+ departments all within a few days.
So, you dial 111 (pencil); the algirithm says 999 (pencil); the paramedic says A&E (pencil); the Triage Nurse says Majors (pencil); the junior Dr says Radiology (4H self-propelling pencil); the senior Dr says Surgery (crayon); the Anaesthetist says GA (tick); the Surgeon says Recovery (eraser); the Recovery Nurse says Ward (coloured pencil); and the Ward Sister gets some fresh paper and a black pen – it’s got to be black – and starts again.
Each of those departments collect information appertaining to their own contribution and relay critical information to one and other as the patient passes through. Just in the typical patient journey described above, imagine the number of Handovers and I haven’t even mentioned primary care.
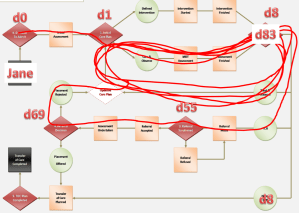
The adjacent flow diagram was part of an audit and shows an MDT decision to ‘go home with domiciliary support’ at Day 8. The decision was a good one, but was followed by lots of bureaucratic faffing about, until at Day 69 some distant committee rejected the decision and by Day 83 Jane Doe died in hospital. One patient amongst many, I presented to a committee… sat in silence.
Continuity of care across big complicated organisations, is certainly a serious business but the clinical decision making seems to have been kidnapped and held hostage, by the bloody paperwork. The best demonstration of the difference between decision making and documentation, is a wad of paper called ‘The Comprehensive Assessment”.

There are hundreds of versions of this bloody thing, usually stretching over 140 pages of forms and boxes and checklists. At the back of that document, there is an equation into which you put all the data, to work out the right answer.
No there isn’t! There’s no sum, no answer at the end, no calculated outcome based on what’s written inside. In fact what most experienced practitioners do – and in the safety of a workshop will admit to straight away with a nervous laugh – is fill in the paperwork to match the decision that they have already made.
And that is completely and unequivocally the right way around. We don’t pay clinicians to fill in forms, we pay them to use all their physical, social, emotional, mental and moral capacities and capabilities, to make bloody good decisions in real time and then, act on them.
The information, augments the decision it does not make it and is best gathered in small increments, as you go along, rather than in one big lump at the end. Or even worse, in a retrospective writing session with some peace and quiet, on your own, in the corner of an office somewhere.
Yet most IT over the past couple of decades, has been obsessed with transferring documentation off bits of paper and onto a screen, in the corner of an office somewhere. In doing so, you mostly lose the advantage of paper (46 inches) and gain none of the advantage of digitising the actual work, as the work is happening.
The focus on documentation is utterly and completely barking up the wrong wooden old tree, when we should be taking every opportunity to digitally transform the critical clinical work of making bloody good decisions. There’s irony for you!
@complexwales
A crap document moved onto a screen, creates a crap screen, filled in retrospect with whatever you happen to remember first. As animals with brains, we rely upon first fit pattern match, not best fit pattern match and that is an acutely situated decision.
Poor design of a document or a screen, can properly bugger up the cognitive processing. Your skull is full of powerful albeit very delicate, wonderfulness, which is why you’ve evolved a thick skull. And we’re back to me, smashing my forehead against things.

Across health and social care and several other partner agencies for that matter, every single day, there are hundreds of thousands of people all engaged in Handover, passing critical information to one and other. Very little of it is captured to validate the next best step. Just in healthcare the people and places and purposes are myriad and interactive and constantly changing.
Typical of a living system of relational and technical exchange, it is possible to make sense of this complexity, by finding and understanding the underlying principles that create the pattern of interaction. When established, those principles transcend the problems of scale in big systems. From one patient on the phone; to a group of patients; several groups in one place; and several places to a whole territory – the underpinning principles simply aggregate, to paint the same picture that can be seen from many different perspectives.
All you need to see it, is a bit of IT to help you zoom in to the detail and out to the context.
A timely example…
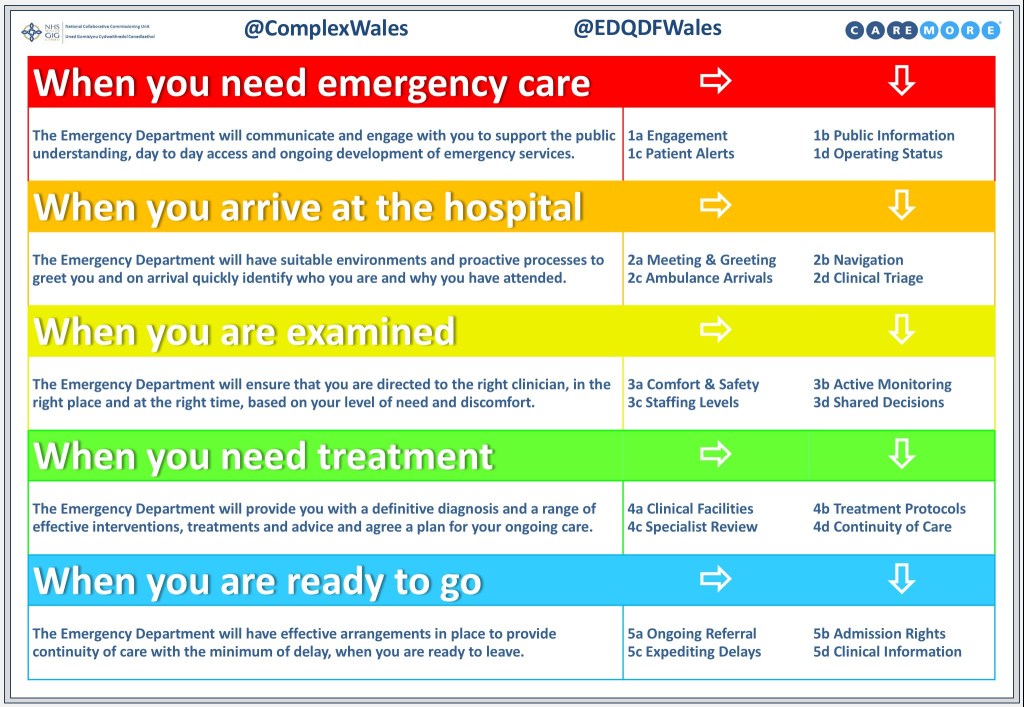
While writing this, it dawned on me that there is a good example of an opportunity to do the right thing, at the right time. Thinking about that pink timeline above, there is a fabulous and eclectic crowd of people from all across the NHS in Wales who have been working on those first few Handovers. More specifically the first face to face contact with the patient, by the call handler virtually, the paramedic at the patient’s home and the nurse when arriving at the hospital door – The Triage.
At the moment NHS Wales has a National Programme developing an Emergency Department Quality & Delivery Framework – transformational work, with a professional network collaborating across thirteen EDs. Ambulance Handover and Triage are integrated into Step 2 of the framework and Pathway Improvement Projects in both are well established. All very good! But in my experience these sorts of things don’t last long and are quickly superseded by the next Shiny idea, so you got to get your wins in quickly.
We have also already got a head start in this area thanks to the Manchester Triage System. There are lots of different versions, but in its most simplistic sense MTS is a numerical scale that helps to align patients into one of five categories – from go home, through minors, specialities, majors and into immediate resuscitation. But the MTS is not used everywhere and not to the same extent.
After all, it’s merely a prioritisation technique, that attempts to sift those in a more life threatening situation straight to the top of the list. It’s a tool (or set of tools) designed for particular problems and therefore has bounded applicability in terms of context: the ‘so what’ of the decision. Every ED is set up slightly differently not just physically as you enter the front door, but also in terms of the variety of services inside the department and the pathways out through the back door.
Two people with the same MTS result may need to go off in two completely different directions. If there was no list, no waiting room, then everyone would be greeted by the highest qualified clinician in the place. Unfortunately, we do not have the time, nor the capacity to have the professor of whatever you’ve broken, waiting for you just inside the door. Unless of course you arrive by helicopter and even then the first thing that happens is a Handover – that started during the flight and is completed as you slide through the door. Honest, it’s that good.
A slight proviso: it’s that good, sometimes, in the highest ranked regional trauma units. Some of them, typically tagged onto the side of a major Emergency Department, have a dedicated lift to a state of the art operating suite and an equally integrated information system. Well, I know of two in the UK and half a dozen in Germany. I’ve also been to an Emergency Department – and a bloody good one – run with a whiteboard by the door. The boss said to me:
“…even the whiteboard is knackered, we have to keep painting it. This is an A&E in the UK in the 21st Century and we are not alone!”
ED CD
Despite this, my colleagues from ED, Ambulance and Primary Care have been engrossed in a deep dive exploring how to align their current practices. They can see the potential for a single continuous process of decision making that enables each new interface to receive and add to the same basic pencil sketch of the patient: a continuous pathway oriented triage. They even drew a proper Model.

Involving primary care will provide a massive head start in the emergency care pathway, with a pretty good picture already sketched out. However, there’s no reason why the telephonist, the paramedic and the triage nurse are not sharing the same picture with the same set of coloured pencils. A very simple bit of existing IT support, could solve that problem this week!
Unfortunately, people are rightly distracted and sorting out a proper Digital Handover during a pandemic seems far from a priority. But I’m deadly serious, this simple continuity in practice is not beyond our reach and will save lives! Particularly right now, when we also have to add to the pathway oriented decision making, the pivotal factor of: COVIDPOS, COVIDNEG & COVIDUKN.
This work must encompass COVID to take advantage of the Tactical opportunity at the moment and take advantage of “technological developments that have been ‘in committee’ for years, suddenly being made available to staff and the public, within a few days”. Albeit that any development cannot be oriented around COVID – dependent upon its peculiarities – or you’ll have to reinvent everything again in a few months and again, every time a new bug shows up.
My only regret is that we didn’t manage to get this in place 2 years ago, when we worked out how pivotal this ubiquitous little Triage moment of decision could be, when faced with a demand that could potentially outstrip our capacity.
The Sweet Spot
The most important attribute of a critical or essential system is that it sustains itself effectively, when it matters most, under the greatest challenge. Bad systems are brittle: they have the characteristic of breaking catastrophically when approaching their limits. Good systems flex, can adapt at their threshold and quickly re-establish their latent pattern, albeit with a tweak or two.
Unfortunately, in the blind pursuit of efficiency, we have too many essential systems and practices that are ignored and undervalued when the pressure is off: gradually and invisibly reducing their adaptive capacity until one day the pressure is back on: like our capability to protect staff, from infectious agents. And we drop the baton!
In a way, my two previous posts on the rules that underpin a Murmuration and how to work beyond complexity in the Tactical domain, have been a foreword to this one – albeit that I didn’t know it at the time. Perhaps this lark was safely residing in the back of my head, as I smashed the front into another wall, frustrated by the reflection of where we could have been with this work by now.
If I knew then, what I know now and all that, but I’ve been deliberately pushed aside for making too much noise and now, on top of everything else, I’m probably getting brain damage, banging my head against a cacophonous lockdown.
But there must be a way to facilitate improving Handover, while the people immersed in the business are at their wits end, with their own excruciating headache. A Digital Handover starting at the front door, is a massive win, for not a lot of work and if anyone can figure out how to get on with it, I promise to amend my previous statement”:
Never a better time to fix something, than just before, it’s properly broken.

Leave a comment